
The 4 Categories of Intravenous Ketamine Usage
As you begin providing intravenous (IV) ketamine infusions or set up your ketamine clinic, you may ask yourself, “How do I determine how far off-label use is still acceptable for IV ketamine use?” Using ketamine to treat mood disorders and chronic pain syndromes is currently considered “off-label,” so how do you know if you are treating another diagnosis that is still safe and scientifically-based? In this blog, we’ll cover the four categories of using ketamine and how it relates to the scientific evidence.
The Four Categories of IV Ketamine Use
First, let’s break down the use of intravenous ketamine into four categories:
“On-label”
“Off-label”
“Super off-label”
“What label”
Let’s take a deep-dive into the four categories in the next section.
“ON-LABEL”
As you probably know, ketamine was FDA approved in 1970 for these clinical indications:
As the sole anesthetic agent for diagnostic and surgical procedures that do not require skeletal muscle relaxation.
For the induction of anesthesia before the administration of other general anesthetic agents.
To supplement low-potency agents, such as nitrous oxide.
Using ketamine in any of the indications above is using it “on-label.” Traditionally, specialties such as anesthesiology and emergency medicine are trained in this type of usage for ketamine.
“OFF-LABEL” USE
Once a drug is FDA approved, doctors can use the medications for a different purpose than originally intended. This has been confirmed by several courts, including the US Supreme Court.
“The United States Supreme Court in Buckman Co. v. Plaintiffs Legal Committee, 531 U.S. 341 (2001), determined that ‘off-label usage’ is ‘accepted and necessary’ by both the FDA and the medical community. Id. at 350. Thus, “[p]hysicians may prescribe drugs and devices for off-label uses.’ Id. at 351 n.5 (citation and quotation marks omitted). Along these same lines, other courts have held that ‘[t]he decision to prescribe such ‘off-label usage’ . . . is regarded as a professional judgment for the healthcare provider to make.’ Nightingale Home Healthcare, Inc. v. Anodyne Therapy, LLC, 589 F.3d 881, 884 (7th Cir. 2009) (applying Illinois law). ‘[D]octors are free to prescribe a drug for off-label use if they deem it medically appropriate for a patient.’ Bennett v. Teva Pharmaceuticals USA, Inc., 2021 WL 797834, at *2 (D. Del. March 2, 2021).” Source here.
Some examples of off-label use would be prescribing quetiapine for insomnia, prazosin for PTSD, propranolol for performance anxiety, colchicine for pericarditis, clomid for male infertility, and modafinil for depression.
Accordingly, researchers have studied the “off-label” use of IV ketamine. This includes research in depression, bipolar disorder, suicidal ideation, anxiety, PTSD, OCD, postpartum depression, acute/chronic pain, and substance use disorder.
Pushing the limits inside of this category would include the serendipitous findings from using IV ketamine in case reports such as priapism, hiccups, or agoraphobia.
“SUPER OFF-LABEL”
Shifting gears into “super off-label” would be diagnoses where there have been no human research trials or case reports, such as amblyopia, tinnitus, PTSD prevention, smoking cessation, or Alzheimer’s disease. There are definitely research opportunities in this category. Furthermore, some promising animal studies have been made already. However, since ketamine is a generic drug, no major pharmaceutical company would have a significant financial interest to invest research funds without long-term patent protection.
“WHAT LABEL”
There is one final area to consider, aka the “what label.” This is the possibility of IV ketamine for certain conditions that have no medical diagnosis. For example, an author who is stuck in writer’s block or an artist seeking increased creativity. Other prospects may be someone seeking psycho-spiritual exploration, curiosity about a near-death experience, recreational use, or possibly even sports-related performance enhancement.
Ketamine Usage and Scientific Evidence
So where does one draw the line? Given that we are operating as a medical clinic within the traditional allopathic paradigm and the fact that ketamine is a Schedule III controlled medication, our approach is to utilize the hierarchy of scientific evidence and limit it to medical usage.
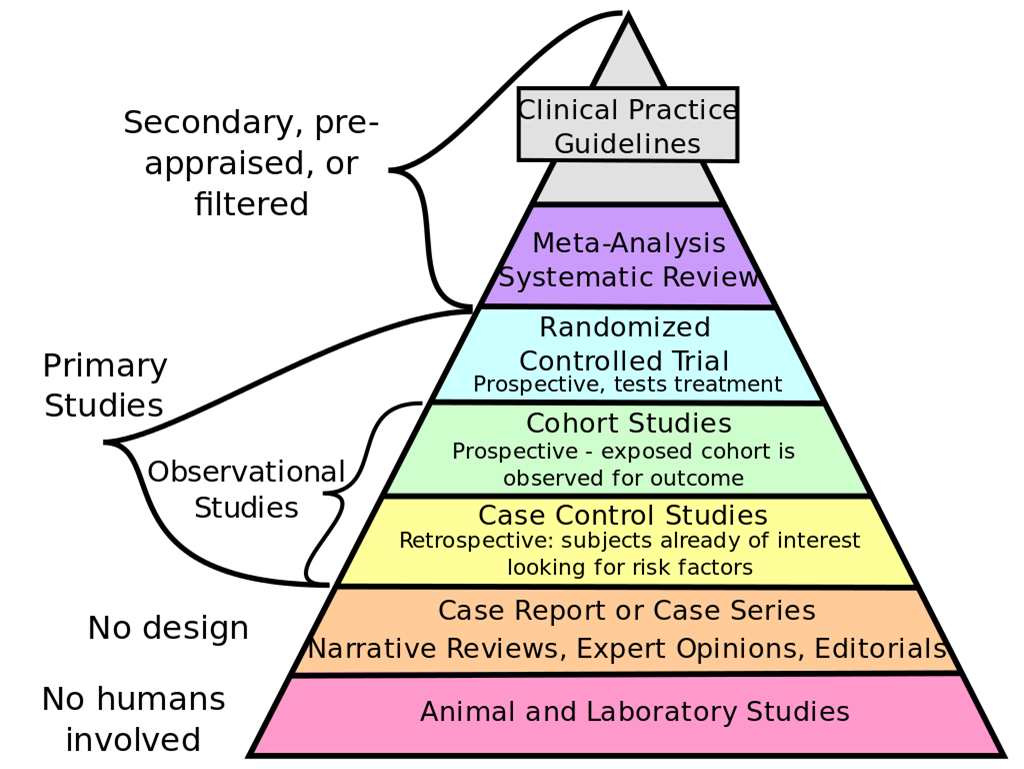
Image Source: https://commons.wikimedia.org/wiki/File:Medical_guide.png
If there is no human research backing up the potential use of IV ketamine, then that would fall under the SUPER OFF-LABEL category. Accordingly, we don’t use it in those cases. Although it could be a ripe area for clinical research, until studies are performed, it would be prudent to use ketamine to treat medical diagnoses that have had designed human studies, i.e. above the case control studies level.
In this traditional allopathic paradigm, we practice evidence-based medicine. Ideally, the evidence would be of the highest quality. For most professionals, using ketamine for “off-label” indications may already be questionable. Therefore, practicing with an evidence-based approach is most pragmatic. For example, if you were ever audited for providing ketamine infusions for depression, you could easily provide the data from scientific articles, but may have some significant challenges for treating amblyopia or writer’s block.
We hope this blog was helpful in exploring this topic of “off-label” usage of ketamine.
If starting a ketamine clinic or adding ketamine infusions to your practice is something you would like to do but aren’t sure how to do so, we can help. Join our email list and be notified about the next free webinar and open registration for Ketamine StartUp.
REFERENCES:
JHP Pharmaceuticals LLC. (2012 March). KETALAR - ketamine hydrochloride injection.
Green, Steven, et al. (2011 May). Clinical practice guideline for emergency department ketamine dissociative sedation: 2011 update. National Library of Medicine. 10.1016/j.annemergmed.2010.11.030
Merelman, Andrew, et al. (2019 April). Alternatives to Rapid Sequence Intubation: Contemporary Airway Management with Ketamine. National Library of Medicine. 10.5811/westjem.2019.4.42753
Bexis (2021, June 21). Can – or Should – State Tort Law Force Defendants To Prevent Off-Label Use? Drug & Device Law.
(2016, January 5). 10 Surprising Off-Label Uses for Prescription Medications. Pharmacy Times.
Lynch, Wendy, et al. (2018 July 24). Efficacy of Ketamine in the Treatment of Substance Use Disorders: A Systematic Review. Frontiers in Psychiatry. https://doi.org/10.3389/fpsyt.2018.00277
Daniel, Park, et al. (2014 July). Ketamine Saves the Day Priapism in a Pediatric Psychiatric Patient. Pediatric Emergency Care, 31(7), 508-510. doi: 10.1097/PEC.0000000000000485
Teodorowicz, J, et al. (1975 July). The effect of ketamine in patients with refractory hiccup in the postoperative period. Preliminary report. Anaesthesia, Resuscitation, and Intensive Therapy, 3(3), 271-272.
Ray, Sheena, et al. (2016 July). Sustained Resolution of Panic Disorder, Agoraphobia, and Generalized Anxiety Disorder With a Single Ketamine Infusion: A Case Report. National Library of Medicine. doi: 10.4088/PCC.15l01899.
Grieco, Steven, et al. (2020 Sep). Subanesthetic Ketamine Reactivates Adult Cortical Plasticity to Restore Vision from Amblyopia. National Library of Medicine. 10.1016/j.cub.2020.07.008.
Bing, Dan, et al. (2015 March). Cochlear NMDA receptors as a therapeutic target of noise-induced tinnitus. National Library of Medicine. doi: 10.1159/000374000.
Brachman, Rebecca. (2017 April). A new class of drug that could prevent depression and PTSD [video]. TED.
Rezvani, Amir, et al. (2018 March). Sub-anesthetic doses of ketamine attenuate nicotine self-administration in rats. Science Direct, 668. 98-102. https://doi.org/10.1016/j.neulet.2018.01.022
Smalheiser, Neil. (2019 July). Ketamine: A Neglected Therapy for Alzheimer Disease. Frontiers in Aging Neuroscience. https://doi.org/10.3389/fnagi.2019.00186

Using ketamine to treat depression and chronic pain is considered “off-label.” What does that mean, and how do you know if you are providing ketamine treatments that are scientifically based? Learn more about this in our blog.








Learn the four critical techniques to ensure patients are both mentally and physically prepared for their sessions, contributing to the success of their care and your ketamine clinic.